Irreducible disc displacement of the temporomandibular joint (TMJ)
What is irreducible disc displacement?
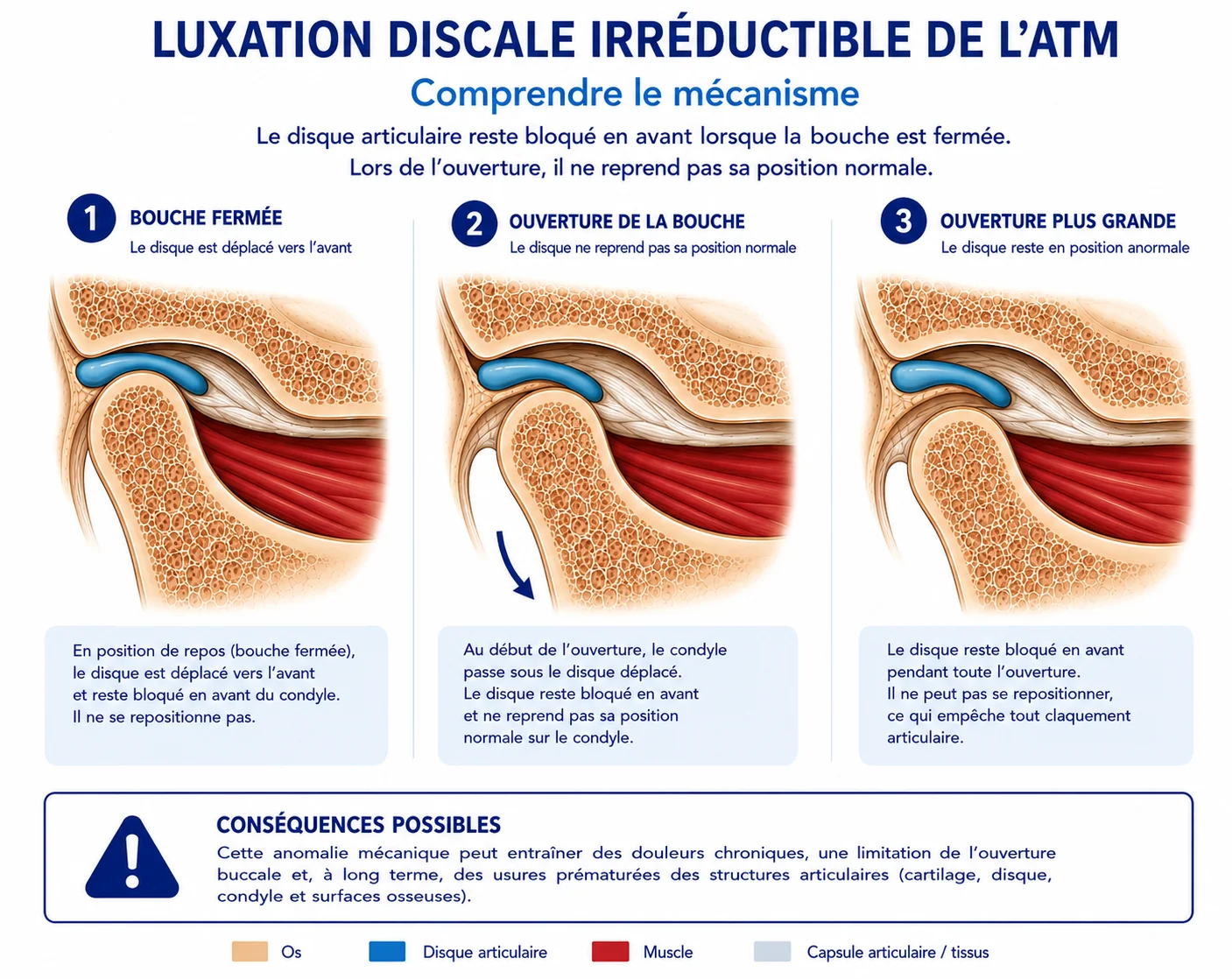
The temporomandibular joint (TMJ) connects the lower jaw to the skull. Between the two articular surfaces lies a small cartilage disc that acts as a shock absorber during jaw movements.
In some people, this disc shifts slightly forward when the mouth is closed. On opening, the joint is unable to move back under this small cartilage disc, resulting in a mechanical blockage. This is known as irreducible disc displacement.
What are the symptoms?
The most common signs are:
- Difficulty opening the mouth fully.
- A feeling of locking on one side.
- Pain in front of the ear and in the jaw, which may radiate to the temples.
- Deviation of the mouth on opening, either to the right or to the left.
- Difficulty eating certain foods, particularly harder foods.
In some cases, the pain may be relatively intense, or absent if the condition is long-standing.
How common is the problem?
Unlike reducible disc displacement, irreducible disc displacement is much rarer. According to studies, it affects around 1 to 3% of the general population.
However, about 5 to 10% of patients who have already had a disc displacement (i.e. reducible disc displacement, with a clicking sound on opening and closing) may experience an episode of irreducible disc displacement during their lifetime, either gradually or suddenly during an acute locking episode.
What should be avoided?
When a joint is painful or irritated, it is advisable to temporarily limit:
- Chewing gum.
- Very hard foods (very crusty baguette, nuts, hard sweets).
- Foods requiring a wide mouth opening.
- Biting on pens, nails or objects.
- Excessive yawning without supporting the jaw.
- Clenching or grinding of the teeth (bruxism) when identified.
Which treatments are recommended?
Current scientific recommendations favour conservative treatments.
Understanding how the joint works often helps to reduce anxiety and the associated muscle tension.
The aim of treatment is to allow mouth opening to improve gradually, with pain decreasing in parallel. A slight limitation may sometimes persist without any serious impact on everyday life.
1. Self-care measures
The following measures are often effective:
- A soft diet during painful periods.
- Limiting extreme opening movements.
- Applying local heat.
- Muscle relaxation exercises.
- Correcting daytime teeth-clenching habits.
2. Specialised physiotherapy
Oro-maxillofacial physiotherapy is crucial here in the treatment, as it will help to:
- Improve mandibular mobility.
- Reduce muscle tension.
- Learn suitable exercises.
- Improve control of jaw movements.
3. Occlusal splint
A splint to be worn at night may be offered in certain situations, particularly when bruxism or nocturnal clenching is present.
Very often, during an acute locking episode, there is a reflex muscle contraction. The aim of a splint is also to restore a comfortable position for the joint at night, a so-called neutral position.
It also aims to reduce muscular and joint stresses. We advise you to consult your treating dentist to have it made.

4. Medication
In cases of significant pain and limitation, your practitioner may temporarily recommend:
- Anti-inflammatories.
- Painkillers.
- Muscle relaxants.
These treatments do not correct the position of the disc but help to reduce inflammation and pain and facilitate jaw mobility.
5. Botulinum toxin injections
In cases where patients have very significant teeth clenching (bruxism: with wear or fractures of the teeth; clenching: clenching only), including at night, the volume of the masseter muscles (in the cheek) can become large and painful.
In some situations, these patients may also prematurely break or damage an occlusal splint. It is therefore recommended to perform botulinum toxin injections to relax the masseter muscles and to avoid excessive pressure on the teeth and joints.
6. Is surgical treatment necessary?
In the vast majority of cases, no.
Surgical or arthroscopic treatments are reserved for particular situations with advanced symptoms.
What is the prognosis?
The prognosis is generally favourable in terms of pain and function, but:
- the disc does not spontaneously reposition itself in the majority of cases
- the joint gradually adapts to new mechanics.
How does the condition progress without invasive treatment?
1. Acute phase: a few days to one or two weeks
Here, the main signs are:
- a very significant limitation of mouth opening
- acute pain, often associated with muscle spasm
In this phase, spontaneous improvement is possible, especially if treatment is started early, combining rest, medical treatment and rehabilitation.
2. Subacute phase: 2 to 8 weeks
Here, the signs are mainly a gradual decrease in pain, with partial recovery of opening. The muscles undergo a degree of adaptation. This is the phase where conservative treatments, such as physiotherapy, are most effective.
3. Chronic phase: beyond two or three months
While pain is often mild or even absent, the patient consults solely because of a limitation of mouth opening, which may be residual but lower than their normal capacity. The disc is generally displaced chronically and the joint has managed to function in an adaptive way.
Repositioning of the disc in the chronic phase is relatively rare, due to adhesions and fibrocartilaginous remodelling. Rehabilitation treatment mainly aims to achieve better function and mouth opening.